Title: Scoping review of challenges faced by female healthcare professionals in the workforce.
Introduction:
Intro and Global data:
The number of women entering the medical and health care workforce globally has increased in the past several decades(Heron, 2016). In Australia, 79% ofwomen are employed inhealth care and social assistance workforce(Statistics, 2018), while in the United States (US) 78% of women work in the healthcare sector(Kirchheimer, 2007).Furthermore, many of female participations are employees in different areas in healthcare sectors, such as medicine, nursing and physiotherapy.In healthcare sectors,such as medicine, nursing and physiotherapy are covered by female participation. For example, in the United Kingdom (UK) more than 90% of the nursing workforce are female (Davey B, 2005; Kirchheimer, 2007), while in Canada it is reported that 40% of physicians are female (Mobilos, Chan, & Brown, 2008) and Australian women make up over one third of Australian medical workforce(Price & Clearihan, 2015).
Women role:
Women have many roles and positions in healthcare organisations, hospitals and healthcare education settings (Lantz, 2008), and include roles such as doctors, nurses, psychiatrists, and administrators.For example, Petek, Gajsek, and Petek Ster (2016) reported that 65% of doctors in Slovenia are women and the ratio of male to female general practice (GP) is 1:5, while in Latvia rate of female doctors is 74.3% (Feldman, 2018).Treister-Goltzman and Peleg (2016) reported that female’s jobs in hospitals were in frontal emergency lines, particularly laboratories and radiological departments. Recently it was reported that 93% of nursing in US was female working in their right area of workforce{Barrett-Landau, 2014 #23469}.
Intro to challenges they may face:
Despite the increase in the number of women in the general workforce, female workers face many challenges in the workplace generally and especially in health care professionals. These challenges include family responsibilities, poor human recourse policies, and gender inequality that hinder their professional growth(Al ‐ Riyami, 2015;Alilu, 2016;Sells, 1989; Treister-Goltzman, 2016). The increase number of women in the health care field and their challenges has drawn special attention to scholars and researchers. For example, work-family balance was highlighted as a significant barrier to career advancement in lots of countries as reported by (K. K. Ali, 2014; Alilu, Zamanzadeh, Fooladi, Valizadeh, & Habibzadeh, 2016; Kerr, Armstrong, & Cade, 2016; Sells & Sells, 1989; Treister-Goltzman & Peleg, 2016).According to Tejas Desai (2016) and Hong Lu (2011) women in the health field face challenges related to a poor work environment which include unequal pay, unsatisfactory working conditions, limited opportunities for career advancement, work-related stress, and unfavourable policies that promote patriarchy.Tejas Desai (2016) reported that women earn less than their male counterparts despite having equal production, amount of work, academic qualification, and experience. Female nurses also been reported to deal with unfriendly workplaces that lack opportunities to advance their career, as well as experience work-family balance challenges that hinder their career progress and affect their lifestyle causing stress and excessive tiredness (Mackusick, 2010 ;Younas, 2014; Kerr, 2016).Previous reports by A. Ali, Subhi, Ringsted, and Konge (2015)show that workplace policies disregard women issues through discriminating female workers via promoting practices. In addition to that, they argue that human resource policymakers have not enacted proper policies to address the gender dynamic differences. These differences (linked with the next paragraph)
To our knowledge there is no recent comprehensive literature review studies that have been undertaken to collectively explore the challenges faced by female health care professionals in the world. Therefore, this study will conduct a scoping review to explore the challenges female healthcare professionals face in the workforce.
Method
The study was conducted as a scoping review approach to allow the researcher to select all available literature for the investigation. A scoping review was used to identify and map the available literature on a selected topic.In this scoping review the researcher used the six methodological steps that conducted by Arksey and O’Malley (2005) framework. The steps are listed as: identifying the research question, identifying relevant studies, selecting studies, charting the data, collating, summarising and reporting the results and consulting experts (Arksey & O’Malley, 2005). The scoping approachsystematically maps and reviews existing literature on a selected topic (Davis et al., 2009), includingliterature from both peer-reviewed and non-peer reviewed literature or greyliterature resulting form (www.greylit.org), Trove and Google Scholar.
- Identify the research question
The research question guiding the scoping review was: What challenges do female health care professionals face in the workforce? This question used all available literature that been published in different disciplines to cover a wide literature in different health care disciplines.
- Identify relevant studies.
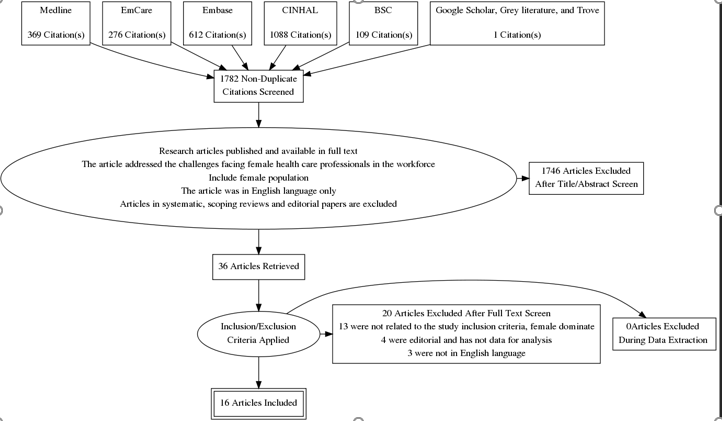
Fivedatabases were used to search for the selected articles: Medline, EmCare, Embase, Cumulative Index of Nursing and Allied Health Literature (CINHAL), Business Source Complete (BSC), Google Scholar, Trove and Grey Literature website www.greylit.org .The search strategy used a list of MeSH terms and text keywords (Table 1). Selected articles were in English only and were filtered from the search yield and the abstract scanned. The databases search were conducted by one researcher (AMA). The search yield resulted 2455 records which were exported to EndNote X8 referencing for screening. The researcher (AMA) removed allduplicates and irrelevant studies and reviewed all relevant abstracts. The selection process was conducted at two levels: a title and abstract review and full-text review. The title and abstract of the selected studies were independently screened (AMA and EK) for inclusion based on existing criteria. In the second stage the selected studies full-text of potentially eligible studies were assessed and inclusion confirmed by two of the authors (AMA and BW). After removing the duplicates, (AMA and BW) conducted the title and abstract review of 1782 articles. After applying the inclusion criteria 36 articles resulted. These 36 articles were reviewed by (AMA & BW) for the second time which ended in 16 articles being included in the scoping review.
Table 1: Search strategy
This table shows the search strategy. The MeSH terms and key words are shown.
|
MeSH:
Challenges
|
MeSH:
Female
|
MeSH:
Health care professionals
|
MeSH:
Workforce
|
|
Keyword:
Barriers
Obstacles
|
Keyword
Women
Gender
Woman
|
Keyword
Healthcare professionals, Allied health, Nurs*, Doctor*, Physician*, Paramedic*, Emergency Medical Services, Emergency Medical Technician*.
|
Keyword
Work-Place
Career
|
- Study selection.
Articles that meet the following inclusion criteria were selected.
- Research articles published and available in full text.
- The article addressed the challenges facing female health care professionals in the workforce.
- Include female population.
- The article was in English language only.
Articles that were systematic and scoping reviews, articles with no abstracts, editorials and letters to editors were excluded.
Read More
- Charting the data
This stage of Arksey and O’Malley framework allows data extraction from the included studies for more data description. A narrative review method was used to extract the data from each study. Narrative reviews summarise studies from which conclusions can be drawn into more holistic interpretation by the reviewers (Kirkevold, 1997). The data included: the author and the year of publication, the country the study was conducted in, the area of the study, the study design or type, the sample size, results and the theme emerges from the study. After full text review of the 16 included articles the researcher developed threethemes which were:i) family responsibilities, ii) Workplace issuesand iii) stereotype-related issues.
- Collating, summarising and reporting the results
The data extracted from the included studies are reported in Table 2.The table summarisesthe selected articles in this scoping review. It presents data on the different opinions that explained the challenges facing female’s healthcare professionals in their workforce. Key outcome data from each of the included studies is presented and include some of the challenges and barriers that face females in their health care workforce. Family responsibilities, workplace issues and stereotype-related issues are the themes whichwere extracted from the literature.
Table 2: studies selected for inclusion.
|
No
|
Author /year
|
Country
|
Discipline
|
Aim of the study
|
Design and Participants
|
Outcomes
|
Theme
|
|
1
|
Sayres M, Wyshark G, Denterlein G, Apfel R, Shore E &Federman D
(1986)
|
UK
|
Medicine
|
To identify possible barrier to women physician who wish to combine with medical careers.
|
Quantitative study by using a questioner sent to the study participants
(n= 56)
|
Pregnancies during residency were common 1:8 married women in 1983 and 77% were usually planned. Seventy-six percent of the women who had been pregnant during residency said that they had received some encouragement from their program directors, and 93% said that they had received some their fellow residents. At the same time, 40% said that their pregnancy had elicited some hospitality from their program directors, and 41% said they had felt some hospitality from their fellow residents.
|
Family responsibilities
|
|
2
|
Barnett RC &Garies KC
(2000)
|
USA
|
Medicine
|
To reduced hours, job-role quality and life satisfaction among married women physician with children.
|
Mixed method by using an interview and 20 minutes survey
(n=104)
|
The main finding of this study of 104 predominantly White, Boston-area, female, reduced-hours physicians in dual- earner couples with children is that subjective reduced- hours job-role quality was a significant predictor of life satisfaction, whereas the number of hours worked per se was not. On average, these reduced-hours physicians experienced more rewards than concerns in their reduced- hours career; after taking into account the number of hours worked, preferred work hours, professional status of spouse, household income, presence of a pre-schooler, negative affectivity, and positive affect, the more positive their subjective experience, the higher their life satisfaction. These results provide support for the expansion hypothesis but not the scarcity hypothesis
|
Family responsibilities
|
|
3
|
Farahat F (2009)
|
Egypt
|
Medicine
|
To explore challenges faced by Egyptian female physician as they pursue their careers and find different ways of coping with these challenges.
|
Quantitative study by using
(n= 300)
|
Challenges reported by physicians were either work or family related. Participating physicians have dealt with challenges in different ways: deciding on a small family size (82.3%), the recruitment of a babysitter/housekeeper (76.3%), and sharing in the family income (62.0%). Selection of potentially nonemergency life style specialist (34.3%), living near the place of work (21%) and taking unpaid vacation (15.7%)
|
Family responsibilities
|
|
4
|
Adisa TA, Mordi C & Mordi T (2014)
|
Nigeria
|
Medicine & Nursing
|
To investigate the challenges and the realities of work-family balance among Nigerian female doctors and nurses in their hysteric efforts to balance their work and family obligations.
|
Qualitative study
(n= 131)
|
The findings thus reveal a number of workplace and domestic problems that threaten female doctors and nurses in their quests for work-family balance. Consequently making work-family strife more pronounced among them. Evidence from the case studies showed that the task of combining multiple roles are very difficult for Nigerian female doctors and nurses. They found the occupational workload of the medical profession all-consuming that they become fatigued and drained and unable to perform their familial duties at the end of their daily shifts.
In Nigeria, the primary responsibility of a woman is to take care of her home and family while every other activity including her job is classified as a secondary role.
|
Family responsibilities
|
|
5
|
Lane N & Piercy N
(2003)
|
UK
|
Nursing
|
To identifies organisational mindsets which militate against women’s career advancement.
|
Mixed method
(n= 43(
|
The study identifies organizational mindsets which militate against women’s career advancement. These mindsets form the basis of the “ethic of discrimination” which both maintains and perpetuates unequal outcomes for women in National Health Service (NHS) nursing. We examine the implications for management in promoting non-discriminatory decision making, and the barriers that are faced in overcoming the “ethic of discrimination”.
|
Workplace issues
|
|
6
|
Baker SR, Barry M, Chaudhry H &Hubbi B
(2005)
|
USA
|
Radiology
|
To determine if the trend of women choosing radiology as a career differs from that for other medical specialities and if there are differences on the basis of the gender of program directors or geographic location.
|
N/M
(n= 186)
|
There was no discernible prejudice against women applicants by program size, location or program director gender.
In both American College of Radiology (ACR) and the Radiological Society of North America (RSNA), women are represented in position of leadership.
Small but increasing number of women chairing academic radiology department.
|
Workplace issues
|
|
7
|
Mobilos S, Chan M & Brown JB (2008)
|
Canada
|
Medicine
|
To examine the experiences of women physicians with regard to the interplay between career and lifestyle choices and to discover how women’s experiences have evolved during the past 3 decades
|
Qualitative study
(n= 12)
|
Three main challenges emerged from the women physicians’ comments: lifestyle and career choices, family planning and career trajectory, and seeking balance.
All participants described the constant struggle they experienced to balanced their personal and professional lives.
|
Workplace issues
|
|
8
|
Nomura K &Gohchi K
(2012)
|
Japan
|
Medicine
|
To investigate whether the experience and the perception of gender-based career obstacles among women in Japan are associated with their working status.
|
Cross-sectional
(n= 1513)
|
being married and having children were significantly associated with part-time practice, indicating that domestic responsibilities still act as strong obstacles that may discourage women physicians from working full-time.
|
Workplace issues
|
|
9
|
Nomura K, Yamazaki K, Gruppen LD, Horie S, Takeuchi M &LllingJ
(2015)
|
Japan
|
Medicine
|
To investigate the difficulties Japanese female doctors face in continuing professional practice.
|
Qualitative
(n= 359)
|
The female doctors reported that professional practice was a struggle with long working hours due to a current shortage of doctors in Japan. Two factors: poor working condition with poor child support, and stereotypical views on gender roles, contributed to a reduction of female doctors in the Japanese workplace and propelled women to switch from full-time to part time work.
|
Workplace issues
|
|
10
|
Price K &Clearihan L (2015)
|
Australia
|
Medicine
|
To explore female general practitioners’ (GPs’) perceptions of possible barriers to leadership and professional roles in the workforce.
|
Quantitative
(n= 30)
|
The top two barriers participants identified for after-hours medical meetings were energy to attend and geographical location. For after-hours care, the top two barriers identified were energy and self-motivation.
|
Workplace issues
|
|
11
|
Phillips J, Hustedde C, Bjorkman S, Prasad R, Sola O, Wendling A, Bjorkman K &Paladine H
(2016)
|
USA
|
Medicine
|
Women family physicians experience challenges in maintaining work-life balance while practicing in rural communities.
|
Qualitative
(n= 25)
|
Women family physicians can build successful careers in rural communities, but supportive employers, relationships, and patient approaches provide a foundation for this success. Educators, employers, communities, and policymakers can adapt their practices to help women family physicians thrive in rural communities.
|
Workplace issues
|
|
12
|
Petek D, Gajsek T & Ster MP (2016)
|
Slovenia
|
Medicine
|
To explore the options and capabilities of women GP specialist trainees in coordinating their family and career.
|
Qualitative
(n= 10)
|
The study results clearly show that the specialist trainees experience a high level of stress at their work, due to the nature of their profession, weaknesses in the health care system, personal traits, inexperience, and interpersonal relations with their colleagues and superiors. An additional burden for them is the needs of their family and/or small children, housework and the obligations of their specialist training.
|
Workplace issues
|
|
13
|
Pfleiderer B, Bortul M, Palmisano S, Rodde S &Hasebrook J (2018)
|
Germany
|
Medicine
|
To improving female physician’s career in academic medicine: chance and challenges
|
Narrative study
|
Shortage of health professional will result in 15% of care services not being delivered because of lack of resources.
The results of the first national survey of female surgeons in Italy conducted on a sample of 167 surgeons (104 women) showed that one of three women (33.7%) reported having suffered sexual discrimination in surgical training, 50% of incidents occurred during their training periods, 29% during job search, and 44% during work. Approximately 30% of a recent sample of women academic clinical medical faculty in the US reported sexual harassment (mostly sexist remarks or behaviour) in their careers, but only 4% of men reported.
Approximately 70% of women perceived gender-specific bias in the academic environment and approximately 66% reported that they personally experienced gender bias in professional advancement.
|
Workplace issues
|
|
14
|
MeghenK,Sweeney C, Linehan C &O’Flynn S
(2018)
|
Ireland
|
Medicine
|
To capture female representation at all level of medicine.
|
Mixed method
(n= N/M)
|
Qualitative finding indicate that females who complete specialist training are a wary of pursuing either flexible training or part time work options and experience discrimination at a number of levels. They appears to be resilient to this and tolerate it. Balancing motherhood and work commitments is the biggest challenge faced by female doctors with children and causes some to change career pathways.
|
Workplace issues
|
|
15
|
Yamazaki Y, Kozono Y, Mori R &Marui E (2011)
|
Japan
|
Medicine
|
To explored the challenges facing Japanese physician-mothers in efforts to identify solutions for their retention.
|
Mixed method
(n= 249)
|
The challenges facing physician-mothers mainly consisted of factors associated with Japanese society, family responsibilities, and work environment. We found that [Japanese Society] epitomized by {traditional gender roles} is a powerful social barrier for female physicians who wish to continue working after they get married and have children. [Family Responsibilities], caring for sick children, feeling guilty about their performance as mothers, and school issues were the main challenges reported by our female physician respondents.
|
Stereotyping related issues
|
|
16
|
Tlaiss H (2013)
|
Lebanon
|
Medicine & Nursing
|
To explore some of the barriers that hinder and the enablers that foster women’s career advancement in the healthcare sector.
|
Qualitative
(n= 10)
|
The results of the study confirm the salience of discriminatory cultural values, gendered social roles and expectations in Middle Eastern societies, and illustrate their role as barriers hindering women’s career advancement. The results also portray the spill over effect of societal expectations and cultural gender stereotypes into the organisational realm, resulting in widely experienced attitudinal and structural organisational barriers. This study reported differences in the illustration of Middle Eastern women to their societies based on their religious affiliation.
|
Stereotyping related issues
|
- Consultation (optional)
After consult and contact tow experts; however no new articles were added after this consultation.
Discussion
This scoping review of challenges faced by female healthcare professionals in the workforce has brought out three broad themes – challenges faced in balancing work and family responsibilities, challenges faced due to workplace issues like lack of supportive policies and gender equality, and challenges faced in stereotyping working women. The 16 literature resources studied for this review have indicated the prevalence of these challenges worldwide, irrespective of geographies and across the various medical roles that women are a part of. Therefore, although the percentage of women joining the healthcare workforce have increased over the years, female workers still have to face many impediments in their work lives that impacts their quality of life both at work and at the home front.
The literature review makes it clear that these challenges are not mutually exclusively, but often overlap with one another at various levels. This means that lack of effective policies (workplace issues) often breed stereotyping issues against working women and disrupt their work-life balance (family responsibilities). Although most of the studies have been categorised under the "workplace issues" theme and a comparatively lesser number of studies bucketed under the "family responsibilities" and "stereotyping related issues" theme, all these are thematically interlinked. The salient understanding in this scoping review is that there are significant challenges prevalent in the healthcare sector for working women, particularly those with children and families.
- Family responsibilities
The 4 articles that are thematically clubbed under "family responsibilities" are geographically separated, based in the UK, the USA, Egypt and Nigeria. However, they are tied with a singular idea that women medical professionals struggle to balance their work and home, being torn between the two opposing expectations of the profession and of the family. Adisa, Mordi & Mordi (2014) clearly identified how a vast majority (95%) of Nigerian female doctors and nurses acknowledged the negative impacts of their medical profession on their family lives, having to thrive in a patriarchal society. The authors noted that a Nigerian woman has to face domestic crises and social sanctions if she prioritises her career over her familial duties. The same work-life conflict prevails among the female physicians of Egypt, who cannot afford time to specialise in their medical career, having to maintain their child rearing and housekeeping duties (Farahat, 2009). At the same time, they face professional ridicule for not having a specialisation.
While the quality of challenge faced by women professionals in Nigeria and Egypt are primarily socio-cultural and in line with the stereotyping related theme, those faced by women in the UK and the USA are mostly workplace related stress. Sayres, et. al. (1986) studied how medical institutions were under-prepared to meet the specific needs of pregnant physicians, sometimes even creating scope for program directors to turn hostile towards their pregnant trainees. Unfortunately, only 22% of the programs had a formal maternity policy, making it more difficult for working mothers to get leaves and other benefits within the institution, mentioned the authors. Barnett & Gareis' (2000) study, however, discussed about the subjective experience of mothers in their medical job roles, which has the final bearing on one's life satisfaction. The authors presented two hypothesis – scarcity hypothesis and enhancement hypothesis – that decide the level of overall fulfilment in the woman physician. As per the scarcity hypothesis, longer working hours mean lesser family time and hence low life satisfaction. And as per the enhancement hypothesis, more roles (both work- and family-wise) mean more rewards and hence higher life satisfaction. This study drew favour for the enhancement hypothesis, although many of the women respondents opted for reduced work hours to resolve their work-family conflict. This could perhaps be explained by the fact that all of the respondents had employed spouses and the entire study is based in a progressive, developed country. Therefore, the familial responsibilities overlap more with the stereotyping issues in the studies based in developing nations, whereas the same overlap with workplace issues in the studies based in developed nations.
- Workplace issues
Long working hours and female physicians opting for flexible work hours or part-time work have been discussed in many studies (Mobilos, Chan & Brown, 2008; Meghen, et. al., 2013; Nomura & Gohchi, 2012; Nomura, et. al., 2015; Phillips, et. al., 2016; Pfleiderer, et. al., 2018). However, reduced work hours, flexible timing and part-time work – all of these attract negative management attitudes in the medical milieu, noted Lane & Piercy (2003). They end up with lower level grades and rarely had career progressions (Lane & Piercy, 2003). Often, women pursuing specialist medical trainings opt for flexi-timing or part-time roles and thereby, attract discrimination from co-workers (Meghen, et. al., 2013; Petek, Gajsek & Ster, 2016). They are considered incompetent for higher roles, just as much as any other female physician or nurse is generally considered incapable in the medical domain. Women are stereotyped as only child-bearing and child-rearing entities, incapable of managerial capabilities (Lane & Piercy, 200; Nomura & Gohchi, 2012; Nomura, et. al., 2015). These are not just workplace issues, but they are also issues related to stereotyping as identified as one of the major themes in this scoping review. Such gender stereotyping sometimes leads to self-silencing on the part of the female physicians, who remain demotivated to even speak in meetings (Price & Clearihan, 2015). These authors attributed such self-silencing to these women's lack of energy and confidence, both stemming from psychological repression at workplaces. This explains why, in spite of 78% of the USA healthcare workforce (Kirchheimer, 2007) and over 90% of the general UK nursing workforce being women (Davey, Murrells & Robinson, 2005), women are underrepresented in leadership positions/roles in the healthcare system, including healthcare organisations, hospitals and medical education institutions (Weil & Mattis, 2003; Eiser & Morahan, 2006; Lantz, 2008). Not just leadership, women are sometimes even missing from specialised roles like diagnostic radiology, studied Baker, et. al. (2005), although the reasons are not related to any of the three themes identified in this document.
Lack of appropriate working conditions prevail and create obstacles to recruiting, retaining and progressing the woman workforce in healthcare (Pfleiderer, et. al., 2018). Justifiably, poor working conditions have adverse psychological effects on the working potential of female doctors and nurses (Nomura & Gohchi, 2012). Therefore, balancing work and gender roles becomes a significant challenge. Some studies also discussed some coping strategies and solutions to the problem. Phillips, et. al. (2016) observed three solutions like reduced/flexible work hours, nurturing supportive relationships and maintaining clear boundaries between personal and professional space and time. While reduced/flexible work hours attract discriminatory attitudes in many contexts, the other two are worthy solutions. Petek, Gajsel & Ster (2016) and Pfleiderer, et. al. (2018) recommended an institutional change, a systemic overhaul with relevant policies (gender equality, family support, active work, maternity, etc). While according to Nomura, et. al. (2015), current employment practices need to be modernised, women must remain committed to achieving career goals, held Meghen, et. al. (2013).
- Stereotype related issues
Although 2 articles have been placed under this theme, many of the other 14 studies, as part of the scoping review, have discussed stereotyping of female physicians and nurses within the gamut of their research. Stereotyping does not exist in isolation and is embedded within the very matrix of the socio-cultural canvas. While some societies and cultures like Japan and the Middle-east demonstrate greater conservatism in terms of a woman workforce, some nations like the US and UK are relatively more open to the idea. Tlaiss (2013) and Yamazaki, et. al. (2011) based their studies in the Middle East and Japan respectively. Both nations are driven by patriarchal, masculine values, whereby domestic responsibilities should be a woman's foremost priority. Therefore, both the studies show how organisational barriers to female doctors are only an extension of the larger socio-cultural expectations from them. To overcome this, these research noted a need for external help (day care, relatives, caregivers, etc.). Sometimes promoting a husband's support in the family is also helpful (Yamazaki, et. al., 2011). However, gender discrimination will never improve unless the local government and authorities come forward and drive an instrumental effort (Tlaiss, 2013).
Conclusion
This scoping review aimed to probe the challenges faced by female healthcare professionals in the workplace. To that end, the six methodological steps given in the Arksey and O’Malley (2005) framework were followed. Finally, 16 articles were shortlisted for review and placed under three broad thematic heads – family responsibilities, workplace issues and stereotyping related issues. Although separated by theme, all of these three themes flow through the articles in a seamless overlap. For example, workplace issues like inadequate women-centric policies lead to work-life imbalance and impact family responsibilities, whereas stereotyping and discrimination again lead to stress, low productivity and low life satisfaction. Low life satisfaction impacts all functions of an individual, both personally and professionally. Then again, professional incompetence due to this dissatisfaction can generate stereotypical thinking that women cannot make good managers and are only responsible for child-rearing. Therefore, all these themes are interconnected and the challenges faced can only be overcome with gradual systemic overhaul, attitudinal changes towards women in general and government-driven anti-discriminatory efforts.
References:
Adamson, B. J., Kenny, D. T., & Wilson-Barnett, J. (1995). The impact of perceived medical dominance on the workplace satisfaction of Australian and British nurses. Journal of Advanced Nursing, 21(1), 172-183. doi:10.1046/j.1365-2648.1995.21010172.x
Ali, A., Subhi, Y., Ringsted, C., & Konge, L. (2015). Gender differences in the acquisition of surgical skills: a systematic review. Surgical Endoscopy, 29(11), 3065-3073. doi:10.1007/s00464-015-4092-2
Ali, K. K. (2014). The Role of Malay Women in the Malaysian Workforce and its Impact on the Consciousness of Ethics and Integrity. Global Business & Management Research, 6(4), 324-333.
Alilu, L., Zamanzadeh, V., Fooladi, M. M., Valizadeh, L., & Habibzadeh, H. (2016). Towards an understanding of clinical nurses challenges that leads intention to leave. Acta Paulista de Enfermagem, 29(5), 534-541. doi:10.1590/1982-0194201600074
Davey B, M. T., Murrells, T., & Robinson S. (2005). Returning to work after maternity leave: UK nurses’ motivations and preferences. Work, Employment, and Society, 19, 327-348.
Eiser, J. A., Morahan, P. (2006). Fixing the system: Breaking the glass ceiling in health care. LIA; 26: 8-13.
Feldman, S. (2018). Female Doctors by Country from The Statistics Portal https://www.statista.com/chart/14983/female-doctors-by-country/
Heron, A. (2016). More women than ever are in the workfore but progress has been glacial. the convewrsation academic rigour, journalist flair.
Hong Lu, K. L. B., Xian Zhang, Alison E. While. (2011). Job satisfaction among hospital nurses revisited: A systematic review. international Journal of Nursing Studies, 49, 1017-1038.
Kerr, H. L., Armstrong, L. A., & Cade, J. E. (2016). Barriers to becoming a female surgeon and the influence of female surgical role models. Postgraduate Medical Journal, 92(1092), 576-580. doi:https://dx.doi.org/10.1136/postgradmedj-2015-133273
Kirchheimer, B. (2007). A woman’s place is in...healthcare, as Modern Healthcare’s Top 25 Women connote explosive growth in the number of female executives in C-suites. Modern Healthcare, 37, 6-7.
Lantz, P. (2008). Gender and leadership in healthcare administration:21st century progress and challenges. Journal of Healthcare Management, 35, 291-.
Mobilos, S., Chan, M., & Brown, J. B. (2008). Women in medicine: the challenge of finding balance. Canadian Family Physician, 54(9), 1285-1286.e1285.
Petek, D., Gajsek, T., & Petek Ster, M. (2016). Work-family balance by women GP specialist trainees in Slovenia: a qualitative study. BMC Medical Education, 16, 31. doi:https://dx.doi.org/10.1186/s12909-016-0551-2
Price, K., & Clearihan, L. (2015). Exploring female GPs' perceptions about medical leadership. Australian Family Physician, 44(6), 399-402.
Sells, J. M., & Sells, C. J. (1989). Pediatrician and parent: a challenge for female physicians. Pediatrics, 84(2), 355-361.
Statistics, A. B. o. (2018). Gender Indicators, Australia, Sep 2018 Retrieved from http://www.abs.gov.au/ausstats/abs@.nsf/PrintAllPreparePage?
Tejas Desai, S. A., Xiangming Fang, Wanda Thompson, pankaj Jawa, Tushar Vachharajani. (2016). Equal work for unequal pay: the gender reimbursement gap for healthcare providers in the United States. postgraduate Medical Journal, 92(1092), 571-575.
Treister-Goltzman, Y., & Peleg, R. (2016). Female Physicians and the Work-Family Conflict. Israel Medical Association Journal: Imaj, 18(5), 261-266.
Weil, P. & Mattis, M. C. (2003). To shatter the glass ceiling in healthcare management: who supports affirmative action and why? Health Services Management Research, 16: 224-33.








