Primary Health Care in Australia
Literature Review
Abstract
Background: The primary healthcare in Australia has been constantly reforming its structure to overcome all the challenges, it was reformed in 2015 by bringing Primary health networks, the understanding of the current challenges may lead to further reforms.
Aim: To assess primary healthcare in Australia.
Design: A qualitative study design was used.
Method: Systematic review was conducted where studies from 2010 to 2020 were selected based on the determined inclusion criteria.
Results: The Primary Healthcare of Australia faces major problems due to the rising stress of chronic illness, an aging population, stresses on the workers, and unsustainable health result inequities and access to services.
Conclusion: Reforms are to be done to the current National primary health care plan and should be focused on Public participation and engagement; keeping Australians healthy; Right time and place of service; innovation in digital and analytics; workforce collaboration plan; funding sources; and collaborations with industries.
Keywords: Australia, Health Care, Primary health care, Systematic Review, Challenges
Introduction
The world health organization describes primary health care as a well-focused approach to managing health determinants and reflects on an inclusive interconnected dimension of overall well-being. Primary health care is the first level of patient care. A Strategy is a plan detailing the vision, goals, and way to proceed with a country to preserve and enhance its citizen’s health status ((Halcomb, Stephens, Bryce, Foley, & Ashley, 2016).). Primary health services should be viewed as both a solution to a health concern faced by community members, as well as a degree of service delivery to community residents. It comes from a wide variety of programs that include health promotion, disease prevention, diagnosis, and chronic illness management. Each individual has the right to good health and wellbeing comes from Article 25 of the universal declaration of human rights (Issel & Wells, 2017).
In a study by McCarthy, Cornally, Moran, & Courtney (2012) they stated that given its relevance to policymakers and more than 30 years of current topic research, the idea of access to healthcare has long been poorly established, without a strong consensus on its interpretation in literature and not a widely agreed way. The meaning and scope of health care itself are issues that have to be discussed in any examination of the concept of access to health care. Alternatively, health care has been used to refer primarily to medical treatment; to a wider spectrum of medical services and secondary non-medical services, from primary care and prevention services to hospital-based tertiary services (Hurley, Baum, Johns, & Labonte, 2010).
There are three types of care programs worldwide: the model for the welfare state, the market model and a combination of the welfare state and the consumer model – the hybrid one. Healthcare is funded by tax funds under the welfare state model, where the government claims sole responsibility for delivering healthcare facilities. Under a market system, it is up to ordinary residents and private institutions to pick and pay for health care. Under a mixed scheme, the state has universal medical benefits so residents can receive private health care in addition to public insurance (Dixit & Sambasivan, 2018).
Australia's health program is a mixed model where Australians, permanent residents, and immigrants can purchase private policies in addition to their current public policies to have access to private as well as public hospitals (Dixit & Sambasivan, 2018). Australia's health infrastructure is regulated by clinics and emergency care services, but it has attracted long-needed criticism since the primary health care field. The publication of the first comprehensive primary health care plan, which acknowledged that for most Australians, primary health care centred in the community is the frontline of health care. The Australian Institute of Health and Welfare has since developed a series of data drive reports which record health system performance against key indicators (Willis, Reynolds, Keleher, (Eds.), 2012).
Objectives
The objective of the study are as follows;
- To assess Primary health care in Australia.
- To review the researches concerning primary healthcare in Australia.
- To discuss the causes and provide a recommendation to overcome challenges in primary healthcare in Australia.
Methods
The research has used a qualitative research design for analysis of primary healthcare in Australia. It used the methods guided by the preferred reporting items for systematic reviews and meta-analyses (PRISMA). For the systematic review, different researches are gathered ranging from 2010 to 2020 (10 years).
Search strategy and data extraction
The study was focused to research the literature which reviews the primary health care of Australia and its constantly changing structure. To determine this the search strategy used keywords like Australia, Health Care, Primary health care, Systematic Review, Challenges. The data was extracted from sources like Google Scholar and PubMed. There were 360 articles on google scholar which were identified, as this was wide-spread combinations of several keywords and modifications were done for more focused research.
Inclusion and exclusion criteria
The steps which were followed were based on the Prisma Flow Chart in Figure 1 where initially 360 articles, where after duplication only 88 remained, further screening lead to 56 studies which led to only 10 studies which were included in the qualitative synthesis which met the complete criteria of the study which meant to be published between 2010 and 2020, with the English language and the abstract should be available for the screening of the research. Further criteria are discussed in Table 1.
|
Inclusion Criteria
|
Exclusion Criteria
|
|
Cohort Study
|
Blogs
|
|
Cross-sectional Study
|
Essays
|
|
Official Government Reports
|
Unofficial Reports
|
|
Case-controlled Study with Comparison or Control Group
|
Websites and Blog
|
|
Studies reporting the Australian primary healthcare sector and its issues/challenges
|
Older versions of the published studies.
|
|
Published from 2010 to 2020
|
Published other than 2010 to 2020
|
Table 1: Inclusion and Exclusion Criteria
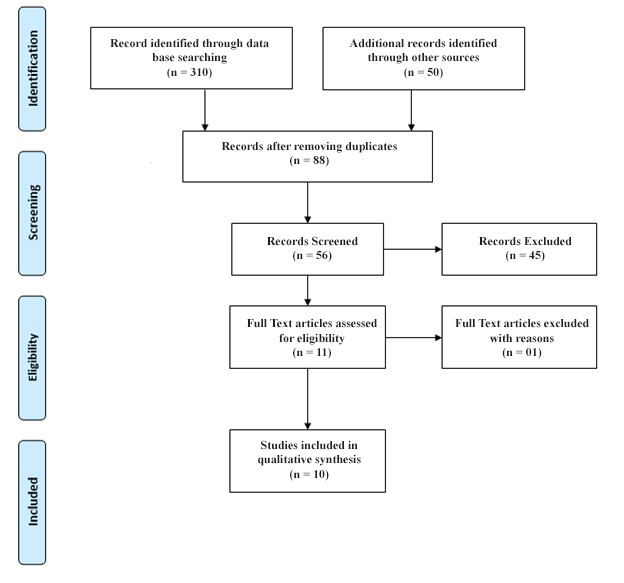
Figure 1: Prisma Flow Chart
Read More
Result
The Australian healthcare system, including the Primary Health Care System (PHC), is structured in a policy model, with shared responsibility for funding and providing services on any level of government. The state or regional government is primarily responsible for primary health care. The Australian healthcare sector is widely regarded in the Organisation for Economic Co-operation and Development sense as one of the best (Briggs, 2017).
Several public and private providers such as general practitioners, community nurses, allied healthcare professionals, mental health professionals, social workers, and Aboriginal and Torres Strait popular health professionals operate in a range of locations providing primary care services. The first point of contact with the health system is in an appropriate setting primary care for a given illness, but the shift in the use of the hospital emergency department, for this reason, was troubling (Willis, Reynolds, & Keleher, 2012; Dixit & Sambasivan, 2018).
The primary health expenditure in 2014-2015 was $56 billion, nearly equal to the $62 billion spent on hospital care. This level of spending which suggests the need for the same degree of primary health care policy funding as hospitals have historically been. Primary health care is a paradigm of community-based provision of health services and the theory of equality and justice in terms of access to reliable, safe, and effective health care. Primary health care is as important for Australia as it is for any nation with low or middle incomes. Australia provides a broad variety of primary health care programs including community health programs, Aboriginal medical services, women's health services, psychological and youth health services (Australia Institute of Health and Welfare, 2016).
The past of Primary health care has been inconsistent, sometimes with inadequate funding for general practices. These concerns resulted in 110 defined geographic regions being formed by the 'Divisions of General Practice.' Subsequently, these divisions were converted into a smaller number of 61 geographically larger organizations called Medicare Locals had a wider reach and had mixed support functions for public health planning. They were more regulated, like General practitioners, other Primary health care clinicians, and 112 community members. Some of the shortest living features of the Australian healthcare cases, which lasted four years after 2011, when Medicare Locals were changing the government was identified as Medicare Locals not surviving. A subsequent study indicated that general practitioners were not sufficiently endorsed and the intent was uncertain. Research in one Australian state nevertheless showed that Medicare Locals were effective in recognizing local needs and establishing strong ties with a variety of partners and medical professionals, in specific general practitioners and health workers associated with them (Briggs, 2017; Horvart, 2014; Javanparast, et al., 2015).
In a study by Dixit & Sambasivan (2018) which deeply shares insights on the key issues and problem, there are selected health system performance indicators where it states that only 10% of the Adult Aussies had to wait for the elective surgeries and about 21% patients reported that there was a coordination issue in the 2 years previously, there were only a few indicators to performance, they also reported that the number of curative care beds was 3.36 to every 1000 people in the year 2013. They also studied that there is a long list for the hospitals, simply put, waiting lists reflect patients who have to wait for medication as recommended by a doctor because of space constraints. In a government-funded healthcare system, waiting queues have a variety of consequences: (a) lengthy waiting lines pose a political headache for policymakers due to the lack of visibility, (b) many people are discouraged from waiting for service at private hospitals, (c) waiting lists are difficult to manage and (d) waiting lists may lead to a lack of use of availableness (Christiansen & Bech, 2013). The number of unique admissions within 28 days of a patient's discharge, divided by the associated cumulative number of separations, is the figure for identified unplanned hospital readmission levels attributable to a postoperative complication. The cost for public hospital separation reported that the average cost per admitted acute weighted separation is 5025 AUD for the year 2014-2015 (Dixit & Sambasivan, 2018). Whereas, in a study by Runciman et al., 2012 which assessed the appropriateness of the health care delivery concluded that while areas of quality and some facets of treatment have been well handled by health providers, there will be continuous progress in the provision of critical patient services and a solution to healthcare disparities. Wide consensus on quality practices is required and the patient records need to be more organized to promote more efficient treatment. The National Primary Health Care strategic framework defined their challenges as getting a stable, integrated primary health care system at its heart is one of the best ways of maintaining a healthy, efficient health system. Readjusting the health system to primary health care would require approaches that help to address some of the difficulties implicit in the Australian health care system, such as fragmentation resulting from the difference between the Commonwealth and state-funded systems, inconsistency in procurement, governance and monitoring arrangements, inadequate coordination of service planning and delivery within the sector (Oliver, 2013; Standing Council on Health, 2013).
Findings
The Australia's health sector faces major problems due to the rising stress of chronic illness, an aging population, stresses on the workers, and unsustainable health result inequities and access to services. It noted that, as much as their clinical needs and conditions, the primary health care services they receive and the quality of treatment that results have relied on where they live, their actual condition and the service providers involved for many people. From a patient viewpoint, there are reports that people tend to be cared for in their own homes and neighbourhoods and that calls for an emphasis on high-quality comprehensive care that makes the diagnosis of patients in the group safer for primary health professionals and scientifically trained experts. There is well-established evidence of considerably lower health outcomes for different Australian groups, including Aboriginal and Torres Strait Islanders, rural and marginal communities, those that are less off-limits, and others with extra or unique health requirements.
Discussion
Australia has a large health network, but there is also room for greater equity, increased services for all; decreased health outcomes variation provided social determinants; changing emphasis from diagnosis to prevention and continually improving the standard of care. The primary health sector for Australia faces significant challenges, including increased costs led by an increasing prevalence of medical diseases, an aging population, unequal access to care and workers and capacity shortages. The shift of patient preferences also points to a desire for more customized, interactive, streamlined and efficient service. Whilst these developments are recognized, suppliers, payers, and larger market actors remain at differing stages of sophistication to respond to the shift — undermining their willingness to improve the framework (Dixit & Sambasivan, 2018). To focus on the future 7 focus areas are identified firstly Public participation and engagement to expand access to knowledge to educate health customers and enhance transparency and to plan and enforce customer confidence-building measures. Secondly, the focus is on keeping people healthy by increase health literacy and changing sentiments for the community through several initiatives. Thirdly, the right time and place matters from the perspective of the community by connecting more communities especially remote ones, setting a standard for the health ecosystem the focus should also be on improving the accessibility and affordability of services in the vicinity of the home. The fourth focus area is increasing innovation, digital, and analytics for the whole system. The fifth focus area is to create a strategic plan for the workforce through collaborations and different pathways. The sixth focus area is to define an outline for outcome-based funding and identify all the sources for possible funding. The last focus area is a pure collaboration with other associated or non-associated industries ("Health Matters", 2020).
Limitation and Conclusion
To conclude this study, restructuring, and reforms for primary health care in Australia are to be done to overcome the current challenges. This study was limited to 10 years, where further studies and wider inclusion can increase the scope of the study, further sub-topics can be studied for a more in-depth analysis of primary health care.
References
Australia Institute of Health and Welfare. (2016). Australia's Health. Australian Government. Retrieved from https://www.aihw.gov.au/getmedia/9844cefb-7745-4dd8-9ee2-f4d1c3d6a727/19787-AH16.pdf.aspx
Briggs, D. S. (2017). Challenges for health systems: Australian perspectives. Public Administration and Policy, 20(1), 6-17.
Christiansen, T., & Bech, M. (2013). Waiting Time Policies in the Health Care Sector. What Works?: Denmark. In OECD Health Policy Studies (pp. 115-131). OECD.
Dixit, S. K., & Sambasivan, M. (2018). A review of the Australian healthcare system: A policy perspective. SAGE open medicine, 6, 2050312118769211.
Halcomb, E., Stephens, M., Bryce, J., Foley, E., & Ashley, C. (2016). Nursing competency standards in primary health care: an integrative review. Journal of clinical nursing, 25(9-10), 1193-1205.
Health Matters. (2020). Retrieved 12 April 2020, from https://www.pwc.com.au/health/health-matters.html
Horvarth, J. (2014). Review of Medicare Locals: report to the Minister of Health and Sport. Canberra: Australian Government.
Hurley, C., Baum, F., Johns, J., & Labonte, R. (2010). Comprehensive primary health care in Australia: findings from a narrative review of the literature.
Issel, L. M., & Wells, R. (2017). Health program planning and evaluation. Jones & Bartlett Learning.
Javanparast, S., Baum, F., Barton, E., Freeman, T., Lawless, A., Fuller, J., & Kidd, M. R. (2015). Medicare Local–Local Health Network partnerships in South Australia: lessons for Primary Health Networks. Medical Journal of Australia, 203(5), 219-219.
McCarthy, G., Cornally, N., Moran, J., & Courtney, M. (2012). Practice nurses and general practitioners: perspectives on the role and future development of practice nursing in Ireland. Journal of clinical nursing, 21(15‐16), 2286-2295.
Oliver, S. J. (2013). The role of traditional medicine practice in primary health care within Aboriginal Australia: a review of the literature. Journal of ethnobiology and ethnomedicine, 9(1), 46.
Runciman, W. B., Hunt, T. D., Hannaford, N. A., Hibbert, P. D., Westbrook, J. I., Coiera, E. W., & Braithwaite, J. (2012). CareTrack: assessing the appropriateness of health care delivery in Australia. Medical Journal of Australia, 197(2), 100-105.
Standing Council on Health. (2013). National primary health care strategic framework.
Willis, E., Reynolds, L., & Keleher, H. (Eds.). (2012). Understanding the Australian Health Care System-E-Book. Elsevier Health Sciences.








