Primary Health Care in Australia | Literature Review
Abstract
Background: The primary healthcare in Australia has been constantly reforming its structure to overcome all the challenges, it was reformed in 2015 by bringing Primary health networks, the understanding of the current challenges may lead to further reforms.
Aim: To assess primary healthcare in Australia.
Design: A qualitative study design was used.
Method: Systematic review was conducted where studies from 2010 to 2020 were selected based on the determined inclusion criteria.
Results: The Primary Healthcare of Australia faces major problems due to the rising stress of chronic illness, an aging population, stresses on the workers, and unsustainable health result inequities and access to services.
Conclusion: Reforms are to be done to the current National primary health care plan and should be focused on Public participation and engagement; keeping Australians healthy; Right time and place of service; innovation in digital and analytics; workforce collaboration plan; funding sources; and collaborations with industries.
Introduction
The world health organization describes primary health care as a well-focused approach to managing health determinants and reflects on an inclusive interconnected dimension of overall well-being. Primary health care is the first level of patient care. A Strategy is a plan detailing the vision, goals, and way to proceed with a country to preserve and enhance its citizen’s health status ((Halcomb, Stephens, Bryce, Foley, & Ashley, 2016).). Primary health services should be viewed as both a solution to a health concern faced by community members, as well as a degree of service delivery to community residents. It comes from a wide variety of programs that include health promotion, disease prevention, diagnosis, and chronic illness management. Each individual has the right to good health and wellbeing comes from Article 25 of the universal declaration of human rights (Issel & Wells, 2017).
In a study by McCarthy, Cornally, Moran, & Courtney (2012) they stated that given its relevance to policymakers and more than 30 years of current topic research, the idea of access to healthcare has long been poorly established, without a strong consensus on its interpretation in literature and not a widely agreed way. The meaning and scope of health care itself are issues that have to be discussed in any examination of the concept of access to health care. Alternatively, health care has been used to refer primarily to medical treatment; to a wider spectrum of medical services and secondary non-medical services, from primary care and prevention services to hospital-based tertiary services (Hurley, Baum, Johns, & Labonte, 2010).
There are three types of care programs worldwide: the model for the welfare state, the market model and a combination of the welfare state and the consumer model – the hybrid one. Healthcare is funded by tax funds under the welfare state model, where the government claims sole responsibility for delivering healthcare facilities. Under a market system, it is up to ordinary residents and private institutions to pick and pay for health care. Under a mixed scheme, the state has universal medical benefits so residents can receive private health care in addition to public insurance (Dixit & Sambasivan, 2018).
Australia’s health program is a mixed model where Australians, permanent residents, and immigrants can purchase private policies in addition to their current public policies to have access to private as well as public hospitals (Dixit & Sambasivan, 2018). Australia’s health infrastructure is regulated by clinics and emergency care services, but it has attracted long-needed criticism since the primary health care field. The publication of the first comprehensive primary health care plan, which acknowledged that for most Australians, primary health care centered in the community is the frontline of health care. The Australian Institute of Health and Welfare has since developed a series of data drive reports which record health system performance against key indicators (Willis, Reynolds, Keleher, (Eds.), 2012).
Objectives
The objective of the study are as follows;
- To assess Primary health care in Australia.
- To review the researches concerning primary healthcare in Australia.
- To discuss the causes and provide a recommendation to overcome challenges in primary healthcare in Australia.
Methods
The research has used a qualitative research design for analysis of primary healthcare in Australia. It used the methods guided by the preferred reporting items for systematic reviews and meta-analyses (PRISMA). For the systematic review, different researches are gathered ranging from 2010 to 2020 (10 years).
Search strategy and data extraction
The study was focused to research the literature which reviews the primary health care services of Australia and its constantly changing structure. To determine this the search strategy used keywords like Australia, Health Care, Primary health care, Systematic Review, Challenges. The data was extracted from sources like Google Scholar and PubMed. There were 360 articles on google scholar which were identified, as this was wide-spread combinations of several keywords and modifications were done for more focused research.
Inclusion and exclusion criteria
The steps which were followed were based on the Prisma Flow Chart in Figure 1 where initially 360 articles, where after duplication only 88 remained, further screening lead to 56 studies which led to only 10 studies which were included in the qualitative synthesis which met the complete criteria of the study which meant to be published between 2010 and 2020, with the English language and the abstract should be available for the screening of the research. Further criteria are discussed in Table 1.
|
Inclusion Criteria |
Exclusion Criteria |
|
Cohort Study |
Blogs |
|
Cross-sectional Study |
Essays |
|
Official Government Reports |
Unofficial Reports |
|
Case-controlled Study with Comparison or Control Group |
Websites and Blog |
|
Studies reporting the Australian primary healthcare sector and its issues/challenges |
Older versions of the published studies.
|
|
Published from 2010 to 2020 |
Published other than 2010 to 2020 |
Table 1: Inclusion and Exclusion Criteria
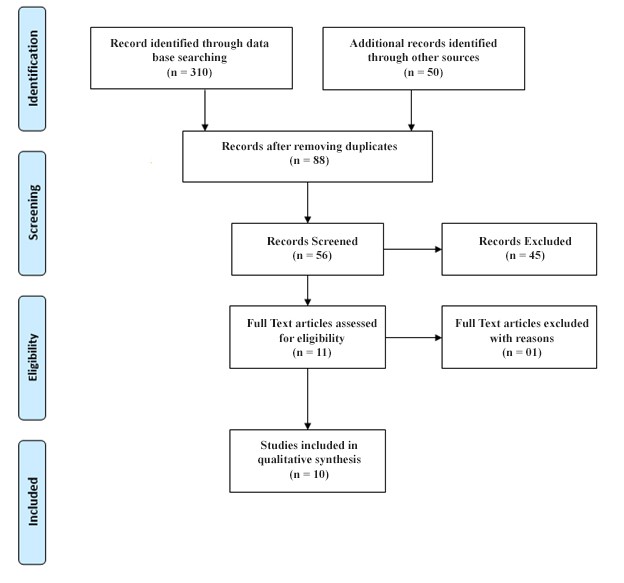
Figure 1: Prisma Flow Chart
Result
The Australian healthcare system, including the Primary Health Care System (PHC), is structured in a policy model, with shared responsibility for funding and providing services on any level of government. The state or regional government is primarily responsible for primary health care. The Australian healthcare sector is widely regarded in the Organization for Economic Co-operation and Development sense as one of the best (Briggs, 2017).
Several public and private providers such as general practitioners, community nurses, allied healthcare professionals, mental health professionals, social workers, and Aboriginal and Torres Strait popular health professionals operate in a range of locations providing primary care services. The first point of contact with the health system is in an appropriate setting primary care for a given illness, but the shift in the use of the hospital emergency department, for this reason, was troubling (Willis, Reynolds, & Keleher, 2012; Dixit & Sambasivan, 2018).
The primary health expenditure in 2014-2015 was $56 billion, nearly equal to the $62 billion spent on hospital care. This level of spending which suggests the need for the same degree of primary health care policy funding as hospitals have historically been. Primary health care is a paradigm of community-based provision of health services and the theory of equality and justice in terms of access to reliable, safe, and effective health care. Primary health care is as important for Australia as it is for any nation with low or middle incomes. Australia provides a broad variety of primary health care programs including community health programs, Aboriginal medical services, women’s health services, psychological and youth health services (Australia Institute of Health and Welfare, 2016).

